Uncategorized
Retatrutide Explained: The Future of Weight Loss
Jun
Retatrutide Explained: The Future of Weight Loss
The Drug That Changed Everything
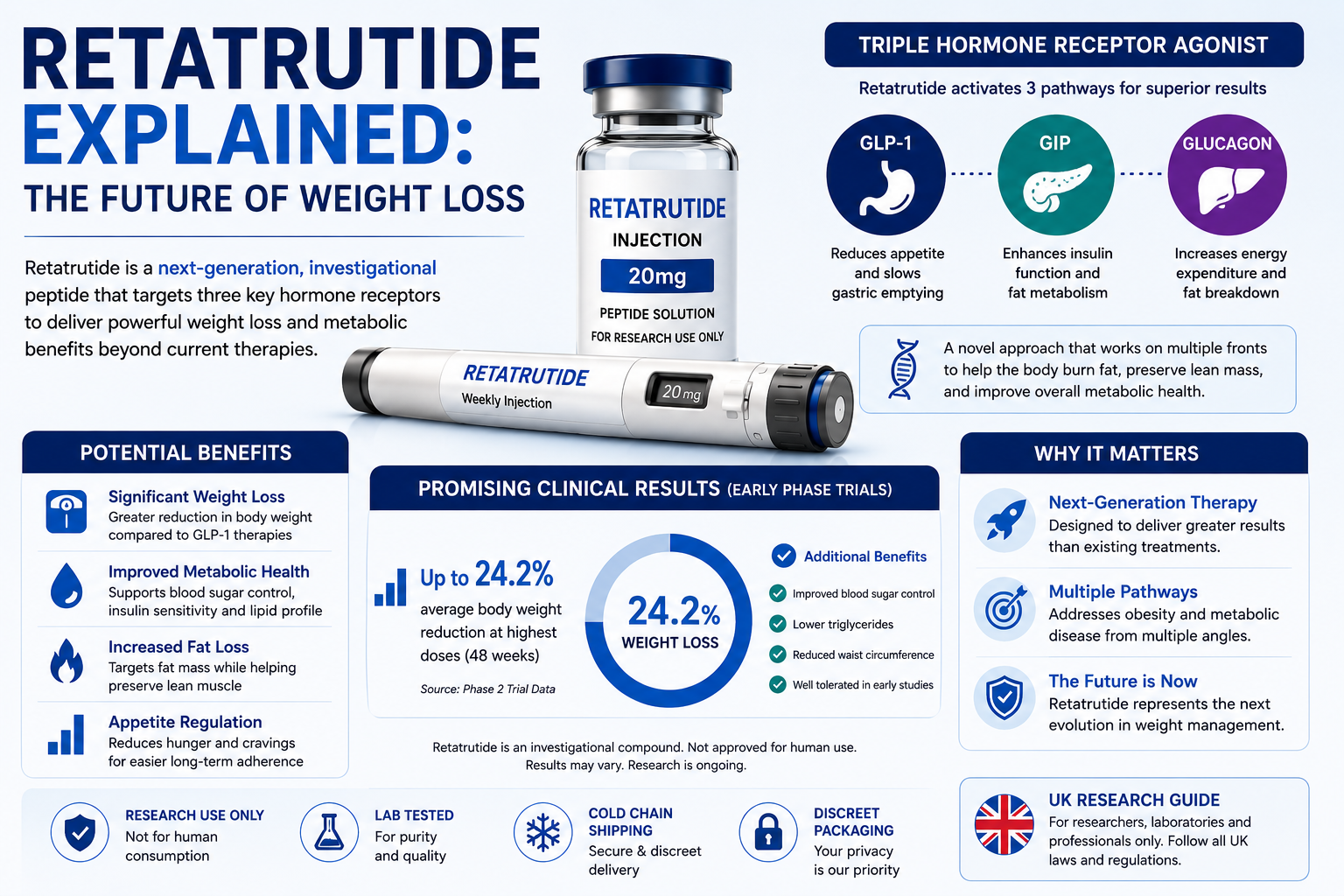
In June 2023, a paper published in the New England Journal of Medicine sent shockwaves through the medical community. Researchers reported that participants in a Phase 2 trial of a new weight loss drug called retatrutide had lost, on average, 24.2% of their body weight over 48 weeks. At the highest dose tested, some participants lost close to a third of their total body weight.
To understand why this was so significant, consider the context. For decades, the medical consensus was that meaningful, sustained weight loss through medication was essentially impossible. The best drugs of the 1990s and 2000s produced modest results — 3 to 8% body weight reduction — and many carried serious side effects. Then came the GLP-1 revolution.
Semaglutide (Ozempic, Wegovy) arrived with results that seemed impossible by old standards: 15% average weight loss. Then tirzepatide (Mounjaro) pushed that to 22%. Now retatrutide appears to have moved the goalposts again — and scientists are beginning to ask a question that would have seemed absurd ten years ago: are we approaching a pharmacological solution to obesity?
📊 Key stat: Retatrutide achieved 24.2% average weight loss in Phase 2 trials — the highest figure ever recorded for a weight loss drug at the time of publication.
The Science: Why Retatrutide Is Different
To understand what makes retatrutide so significant, you need to understand the hormonal systems it targets — and why hitting three simultaneously is such a departure from what came before.
A Brief History of Weight Loss Drug Mechanisms
Early weight loss drugs worked primarily by suppressing appetite through the central nervous system or by blocking fat absorption in the gut. They were blunt instruments. The real breakthrough came when researchers began studying incretin hormones — gut-derived peptides that regulate blood sugar and appetite.
GLP-1 (Glucagon-Like Peptide-1) was the first incretin to be successfully targeted. When GLP-1 is activated, it stimulates insulin release, slows digestion, and — critically — signals the brain to reduce hunger. The result was a new class of drugs that worked with the body’s own hormonal systems rather than overriding them.
Retatrutide’s Triple Mechanism — Explained Simply
Mechanism 1: GLP-1 Receptor Agonism — Hunger Control
Like semaglutide and tirzepatide, retatrutide activates GLP-1 receptors. This suppresses appetite by acting on the hypothalamus, slows gastric emptying so you feel full longer, and improves insulin sensitivity. This is the foundation all modern weight loss injectables share.
Mechanism 2: GIP Receptor Agonism — Metabolic Enhancement
GIP (Glucose-Dependent Insulinotropic Polypeptide) amplifies the effects of GLP-1 activity, improves fat cell metabolism, and reduces some gastrointestinal side effects that pure GLP-1 drugs produce. Adding GIP is a significant part of why tirzepatide outperforms semaglutide.
Mechanism 3: Glucagon Receptor Agonism — The Game Changer
This is what separates retatrutide from everything before it. Glucagon receptor activation dramatically increases energy expenditure — essentially turning up the body’s metabolic rate while simultaneously reducing calorie intake through GLP-1. You are burning more and eating less through two entirely separate biological pathways.
Additionally, glucagon receptor agonism appears to specifically target fat stored in the liver — a major concern in non-alcoholic fatty liver disease (NAFLD), which affects an estimated five million people in the UK.
🔬 In plain English: Retatrutide makes you less hungry (GLP-1), improves how your body handles fat (GIP), and increases how much energy your body burns at rest (Glucagon). Three jobs that previous drugs could only do one or two of.
The Clinical Trial Data: What We Know So Far
Phase 2 Trial — The Landmark Results
The Phase 2 trial enrolled 338 adults with obesity (BMI 30–50) without type 2 diabetes. Participants received one of five weekly doses of retatrutide or a placebo over 48 weeks, alongside lifestyle counselling.
Results published in the New England Journal of Medicine (June 2023):
- 1 mg dose: ~8.7% average weight loss
- 2 mg dose: ~17.3% average weight loss
- 4 mg dose: ~19.3% average weight loss
- 8 mg dose: ~22.8% average weight loss
- 12 mg dose: ~24.2% average weight loss
- Placebo: ~2.1% average weight loss
Notably, weight loss had not plateaued by week 48 in the higher dose groups — suggesting continued treatment beyond one year could produce even greater results, a pattern not seen as clearly with earlier drugs.
Secondary Benefits Observed
Beyond the headline weight loss, the trial recorded significant metabolic improvements:
- Meaningful reductions in waist circumference
- Improvements in blood pressure
- Reduction in triglyceride levels
- Reduction in liver fat content (MRI-confirmed in a subset)
- Improvements in blood sugar regulation
Phase 3 Trials: What Is Being Tested Now
Eli Lilly launched a comprehensive Phase 3 programme — the TRIUMPH trials — covering multiple patient groups:
- TRIUMPH-1: Obesity without type 2 diabetes (primary weight loss indication)
- TRIUMPH-2: Obesity with type 2 diabetes
- TRIUMPH-3: Cardiovascular outcomes in high-risk patients
- Additional trials: NAFLD/MASH (liver disease)
Results from the primary trials are expected in late 2025 to 2026. If they confirm Phase 2 findings at scale, the scientific case for approval will be extremely strong.
Development Timeline: From Lab to UK Pharmacy
| Year | Milestone | Significance |
| 2019–2021 | Preclinical development at Eli Lilly | Triple agonist concept validated in animal models |
| 2022 | Phase 1 safety trials begin | First human dosing; safety and pharmacokinetics established |
| 2022–2023 | Phase 2 efficacy trials | 48-week trial; 24.2% average weight loss at highest dose |
| 2023 | Phase 2 results published (NEJM) | Landmark publication triggers global interest |
| 2024–2026 | Phase 3 trials underway | Large-scale trials across multiple countries incl. UK sites |
| Late 2026 (est.) | Phase 3 results expected | Will determine regulatory submission timeline |
| 2027+ (est.) | Potential MHRA/FDA approval | Subject to Phase 3 success and regulatory review |
The timeline above represents the most optimistic realistic scenario. UK residents should treat 2027 as an earliest possible date, with 2028–2029 as a more conservative estimate.
How Does Retatrutide Compare to Current Options?
| Drug | Receptors | Avg. weight loss | Frequency | UK status |
| Retatrutide | GLP-1 + GIP + Glucagon | ~24% (Phase 2) | Once weekly | Not approved |
| Tirzepatide (Mounjaro) | GLP-1 + GIP | ~22% | Once weekly | MHRA approved ✓ |
| Semaglutide (Wegovy) | GLP-1 | ~15% | Once weekly | MHRA approved ✓ |
| Liraglutide (Saxenda) | GLP-1 | ~8% | Once daily | MHRA approved ✓ |
| Orlistat | Lipase inhibitor | ~3–5% | 3x daily pill | MHRA approved ✓ |
Each generation of weight loss drugs has roughly doubled average weight loss achieved. If retatrutide’s Phase 3 results confirm Phase 2 data, it will represent the most significant single advance in weight loss pharmacology to date.
What Retatrutide Could Mean for the UK
The Scale of the Obesity Challenge
More than 26% of adults in England are classified as obese, and a further 38% are overweight (NHS Digital). The NHS spends an estimated £6.5 billion per year on obesity-related conditions. Effective pharmacological treatment at scale could have enormous public health and economic implications.
A Shift in How We Think About Obesity
Perhaps the most important implication of drugs like retatrutide is cultural and scientific. For decades, obesity was viewed — including by some medical professionals — as primarily a matter of willpower. The success of GLP-1 drugs has forced a reassessment: obesity is a complex metabolic condition with identifiable hormonal drivers, and it responds to medical treatment in ways that diet and exercise alone rarely achieve sustainably.
Retatrutide, if approved, will reinforce this shift. The prospect of 24% average weight loss through a once-weekly injection — alongside improvements in cardiovascular markers, liver health, and blood sugar — will be difficult to frame as anything other than a serious medical breakthrough.
The NHS Access Question
One of the biggest challenges retatrutide will face in the UK is not regulatory but economic. NICE must determine whether the drug represents value for money for the NHS. Given the ongoing backlog for existing GLP-1 drugs and supply chain challenges, widespread NHS access — even after approval — may take additional years. Private prescriptions will likely be available sooner, at an estimated £200–£350+ per month.
Legitimate Concerns and Open Questions
Responsible coverage requires acknowledging what Phase 3 has yet to confirm:
Long-term safety beyond one year
Phase 2 trials ran for 48 weeks. We do not yet have robust data on two, five, or ten years of continuous use. The cardiovascular outcome trial (TRIUMPH-3) will be critical.
Weight regain after stopping
This is the most consistent challenge across the GLP-1 class. When patients stop semaglutide or tirzepatide, substantial weight regain typically follows within one to two years. There is no reason to assume retatrutide will be different — which raises long-term cost and health questions.
Glucagon component and muscle mass
Some researchers have raised questions about whether glucagon receptor activation might accelerate loss of lean muscle alongside fat. Early trial data did not show significant muscle loss, but longer-term monitoring is needed.
Thyroid concerns
GLP-1 drugs carry a class warning regarding thyroid C-cell tumours based on animal studies. No increased thyroid cancer signal has been detected in human trials to date, but adding glucagon agonism introduces a new variable regulators will scrutinise carefully.
✅ The honest assessment: The early data for retatrutide is genuinely impressive. But impressive Phase 2 data does not guarantee Phase 3 success, and Phase 3 success does not guarantee a clean long-term safety record. Scientific caution is warranted alongside genuine excitement.
What Should UK Residents Do Right Now?
If You Need Help With Weight Management Now
Do not wait for retatrutide. There are highly effective, MHRA-approved options available today. Speak to your GP about referral to an NHS weight management service, or explore private options. Mounjaro (tirzepatide) in particular offers results very close to what retatrutide has shown — available now, safely, through regulated channels.
If You Want to Stay Informed on Retatrutide
- Bookmark ClinicalTrials.gov and search ‘retatrutide’ for trial updates
- Monitor Eli Lilly’s investor relations page for Phase 3 announcements
- Watch the MHRA’s ‘new medicines’ section at gov.uk
- Follow the New England Journal of Medicine and The Lancet for peer-reviewed results
If You Are Considering Grey-Market Sources
Please do not. Risks include counterfeit products, incorrect dosing, contamination, and no medical oversight. The regulated alternatives available today are both safer and genuinely effective. The wait for retatrutide is worth it if your goal is safe, sustained weight loss.
Conclusion: A Genuine Turning Point
Retatrutide is not hype. The science behind its triple-receptor mechanism is sound, the Phase 2 data is the strongest ever seen for a weight loss drug, and the researchers behind it are among the world’s leading experts in metabolic medicine. If Phase 3 confirms what Phase 2 suggested, we will look back on this period as a genuine turning point in how medicine approaches obesity.
But turning points take time to arrive fully. For UK residents, the realistic horizon for accessing retatrutide through safe, regulated channels is 2027 at the earliest. In the meantime, the approved options available today are better than anything that existed five years ago. The future is coming. The present is already pretty good.